What is Autosomal Dominant Inheritance?
-
 Ravi Kiran Reddy
Ravi Kiran Reddy
- 2 years ago
- 0 Comments
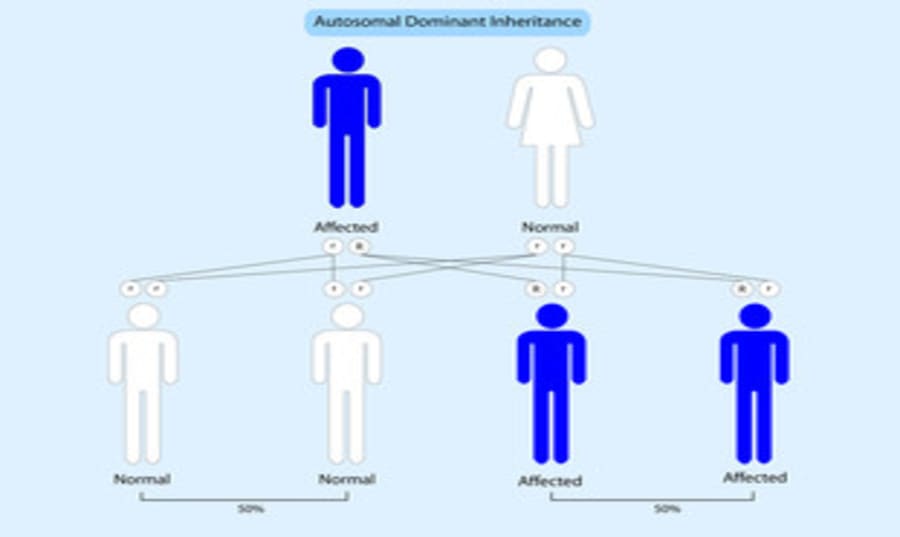
Autosomal Dominant Inheritance:
Although, in theory, autosomal dominant inheritance is the simplest model for genetic counselling, in practice it provides some of the most difficult problems, with traps for the unwary that require special mention. An autosomal dominant disorder or trait can be defined either by the observed pattern of transmission between generations in families or as one that is largely or completely expressed in the heterozygote.
The homozygous state is either unknown or excessively rare in dominantly inherited disorders, but when it does occur it is usually much more severe than the normal heterozygous form (e.g. familial hypercholesterolaemia) or lethal (e.g. achondroplasia). In Huntington’s disease, however, the homozygote appears to be a little different from the heterozygote, so this is one of the few cases known to fit both definitions.
In its fully developed form, the pattern of autosomal dominant inheritance is characteristic and allows precise risks to be given The risk to offspring of affected members will be one half (i.e. 50%, one in two, or with an odds ratio of regardless of sex and regardless of whether the disease is fully developed or sub- or pre-clinical. The risk for offspring and more distant descendants of unaffected family members is not increased over the general population risk, provided that the individual really is unaffected.
Problems arise from the variability of gene expression that is seen in many dominantly inherited disorders and which, until recently, has not been understood to any significant extent. The uncovering of the molecular basis of some of this variability is proving to be one of the most interesting fields of human genetics, as well as helping to resolve the practical problems encountered in genetic counselling.
Homozygosity in autosomal dominant disease:
Almost all patients seen with autosomal dominant conditions will be heterozygotes, having inherited their disorder from only one side of the family or representing new mutations. Homozygosity requires both parents to have transmitted the mutated gene; this is most unlikely to happen unless one of the following is the case:
- The gene is common and relatively mild or late-onset in its effects.
- Two affected individuals have married one another.
Familial hypercholesterolaemia provides an example of the first situation; the heterozygote frequency may be as high as 1 in 500, so one might expect chance marriages between such individuals to occur with a frequency of 1 in 250,000. Since only a quarter of the offspring of such a couple would be homozygous, one would expect the frequency of homozygotes to be only one in a million, and they are indeed exceedingly rare. Consanguinity would, of course, increase the chance of homozygosity, exactly as in autosomal recessive inheritance.
The situation more likely to be met in a genetic counselling clinic is where two individuals with the same disorder marry preferentially. This is seen not infrequently in achondroplasia; the risks for the offspring in such a situation will be one-quarter homozygous affected, one-half heterozygous achondroplasia, and one-quarter unaffected.
In achondroplasia, the affected homozygote usually dies rapidly after birth owing to the constricted chest; in most other dominant disorders the homozygous condition is likewise very severe or lethal. In the case of Huntington’s disease, no such differences have been observed, even though a number of marriages between heterozygotes are recorded; molecular analysis of the offspring has now confirmed that the homozygote may be indistinguishable from the heterozygote.
A somewhat similar (though rare) situation may occur when marriage partners have different but allelic, disorders. The child may then receive both abnormal alleles and will appear as a ‘genetic compound’. This has been recorded with achondroplasia and milder dysplasia.
X-LINKED DOMINANT INHERITANCE:
The pattern may at first glance be mistaken for autosomal dominant inheritance but, if the offspring of affected males are considered, all sons are unaffected and all daughters are affected. The excess of affected females can also be seen.
INTERMEDIATE X-LINKED INHERITANCE
The blurred distinction between dominant and recessive in X-linked disease has already been mentioned. In a few conditions, heterozygotes may show the disease in one branch of a family, but not in another. Although at first sight, the pattern appears confusing, the situation is soon clarified if the offspring of affected males are considered – all sons are unaffected, while the females are either affected or carriers.
X-LINKED DOMINANT INHERITANCE WITH THE ABSENCE OF AFFECTED MALES
In a number of disorders, the condition is seen only in the heterozygous females, the affected (hemizygous) males being undetected or appearing as an excess of spontaneous abortions. It is difficult to prove this situation, but it has now been confirmed for several disorders, including focal dermal hypoplasia and incontinentia pigmenti but (in contrast to earlier ideas) does not apply to Rett syndrome.
Genetic counselling risk estimates in these circumstances require some care. Leaving aside spontaneous abortions, one-third of the offspring of an affected woman will be affected; all the live-born males will be unaffected, as will half of the females. Two-thirds of all offspring will be female. If the pattern of inheritance is clear but the mutation unknown, fetal sexing with the termination of female pregnancies may be a possibility, at least in theory. Where an affected child has been born to healthy parents, this is likely to represent a new mutation and the recurrence risk is likely to be low (most such patients will be female).
Another reason for the absence of males in a disorder caused by dominant mutations in a gene on the X chromosome is when affected females do not reproduce and the mutational origin of the disease is predominantly at spermatogenesis so that it almost always manifests in an affected female. This is the case in Rett syndrome, although males can be affected by this if they have Klinefelter syndrome (47, XXY) or if they are somatic mosaics for the causal MECP2 mutation.
A male with a MECP2 gene mutation that would cause Rett syndrome in a female is usually affected by a substantially more severe, neonatal-onset encephalopathy without the period of apparently normal development for 6 months or more that is found in Rett syndrome. A similar but less marked preponderance of affected females can arise in other sex-linked disorders if the fertility of affected females is reduced and the origin of mutations is predominantly at spermatogenesis (as in craniofrontonasal dysplasia) but may also be post- zygotic in mosaic females.
COMMON X-LINKED DISORDERS
Where an X-linked gene is common in a particular population, confusing pedigree patterns may be produced. This may be seen with red-green colour-blindness in European populations and with glucose-6-phosphate dehydrogenase deficiency in the Middle East and many parts of Asia. The marriage of affected males to heterozygous females is not infrequent and will result in homozygous females all of whose sons will be affected. A similar pattern can occasionally be seen with less common disorders when there is consanguinity.
Risk of being a carrier for an X-linked disorder:
Methods of carrier detection in X-linked disorders are discussed, but it is clearly important to estimate the genetic risk of a female relative being a carrier, so that information from carrier testing (if any) can be appropriately combined with the risk from family structure (i.e. the risk from the pedigree). The estimation of these risks is not always easy and is one of the situations where a mathematical approach is needed in genetic counselling. Young’s Introduction to Risk Calculation (see ‘Further Reading’) is strongly recommended for this and other areas of risk estimation.



Leave Comment